PO.CL04.02 · 临床研究
Transcriptomic landscape for African-specific low-grade prostate cancer
作者与单位 Authors & Affiliations
摘要 Abstract
BACKGROUND
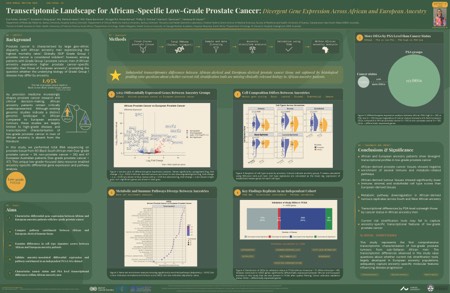
Prostate cancer (PCa) is characterized by large geo-ethnic disparity, with African ancestry being a recognized risk factor of aggressive disease. Globally, ISUP Grade Group 1 (GG1) PCa is considered indolent and is typically treated with active surveillance rather than active treatment. However, this approach is unfeasible in Sub-Saharan Africa due to limited access to PSA testing, imaging, and repeat biopsies. Moreover, ISUP grading developed in European ancestral populations may not reflect African PCa biology.
AIM
This project aimed to explore transcriptional differences between African and European ancestral men presenting with GG1 PCa.
METHODS
Focusing on men from Southern Africa, we performed total RNA sequencing of fresh-frozen (FF) diagnostic prostate biopsy samples from 60 African men with either GG1 PCa (n=28) or without PCa (non-PCa, n=32). FF prostatectomy samples from 47 Australian men of European ancestry with GG1 PCa were sequenced in parallel. This unique data resource enabled ancestry-specific differential gene expression and pathway analysis.
RESULTS
Principal component analysis of the top 1000 most variably expressed genes showed no clear separation between PCa and non-PCa; however, we observed a clear separation between South African and European men. From 24,008 genes, 4,641 were differentially expressed (DE) between African and European-derived GG1 tumors ( P < 0.05, BH-adjusted). The top 5 candidate genes included downregulation of the tumor suppressor JUN in African ancestral tumors. Gene set enrichment analysis (GSEA) of all 24,008 genes and overrepresentation analysis (ORA) of the significant DE genes revealed downregulation of several immune and metabolic pathways ( P < 0.05, BH-adjusted, NES < -1), indicative of more aggressive PCa driven by unique molecular pathways. Cell type analysis demonstrated lower immune cell, stromal cell, and angiogenesis scores in African compared to European-derived tumors, with stromal cells and angiogenesis reaching statistical significance ( P -value < 0.05). The latter indicative of a less diverse tumor microenvironment in African PCa.
Analysis of African ancestry PCa vs. non-PCa identified only 12 DE genes ( P < 0.05, BH-adjusted). The limited number of significant genes after adjustment may reflect the small sample size or undetected disease in the non-PCa group, which would reduce contrast between the groups. However, GSEA and ORA showed upregulation of proliferative pathways and androgen response ( P < 0.05, BH-adjusted, NES > 1), which is the expected pattern of PCa vs. non-PCa.
CONCLUSIONS
In this first-of-its-kind study, we reveal distinct transcriptomic profiles between prostate tumors derived from men of African vs. European ancestry. Our results suggest that current active surveillance strategies may not be safe for African ancestral patients with GG1 PCa.
利益披露 Disclosure
E. F. Jensby, None..
K. Uthayopas, None..
M. Hasan, None..
R. Bornman, None..
S. B. A. Mutambirwa, None..
P. D. Stricker, None..
K. D. Sørensen, None..
V. M. Hayes, None.