PO.IM01.11 · 免疫学
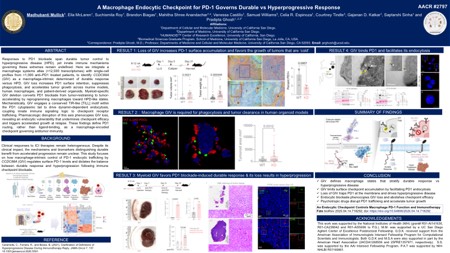
A macrophage endocytic checkpoint for PD-1 governs durable vs hyperprogressive response
作者与单位 Authors & Affiliations
摘要 Abstract
Clinical responses to PD-1 blockade span a wide continuum, from durable regressions to hyperprogressive disease (HPD); yet the macrophage-intrinsic switches that determine these extremes responses remain undefined. Using a macrophage systems model built from >12,500 transcriptomes and calibrated with single-cell transcriptomes from >1,000 anti-PD-1-treated patients, we identified CCDC88A (encodes the endocytic adaptor, GIV) as a top responder-linked gene and mechanistic driver of tumor-associated macrophage (TAM)states predictive of clinical benefit versus HPD. Loss of GIV in macrophages increased cell-surface PD-1 across species and platforms (primary cell-line, and organoid co-cultures), impaired phagocytosis, and accelerated tumor progression. In syngeneic models, myeloid-specific GIV deletion converted anti-PD-1 therapy from tumor-controlling (beneficial) to tumor-accelerating (hyperprogressive), without altering T cell targeting; transcriptomic analyses of tumor-infiltrating myeloid cells confirmed a shift towards HPD-associated macrophage signatures. Mechanistically, GIV engages a TIR-like BB-loop (TILL) motif within the PD-1 cytoplasmic tail and functions as an endocytic adaptor, driving dynamin-mediated PD-1 internalization and recycling. A pharmacogenomic perturbation strategy revealed that blocking endocytic trafficking phenocopies GIV loss both in vitro and in vivo : PD-1 is trapped on the TAM surface, checkpoint blockade fails, and tumors accelerate under therapy. Conversely, preserving GIV•PD-1 coupling enhances response durability. Finally, we uncover a clinically relevant vulnerability: FDA-approved psychotropic and antiemetic drugs that impair receptor internalization (e.g., prochlorperazine) negate anti-PD-1 efficacy and induce HPD-like progression in vivo , consistent with pharmacoepidemiologic evidence linking such drugs to increased mortality and immune-related adverse events in patients receiving checkpoint therapy. Collectively, these findings establish GIV-dependent PD-1 routing as a macrophage-encoded checkpoint that dictates whether PD-1 blockade elicits tumor clearance or fuels malignant outgrowth. By repositioning TAMs as active arbiters of immunotherapy fate, this work exposes PD-1 trafficking, and its drug-induced derailment, as a new axis for therapeutic control and precision risk mitigation in solid tumors.
利益披露 Disclosure
M. Mullick, None..
E. McLaren, None..
S. Roy, None..
B. Biagas, None..
M. Anandachar, None..
V. Castillo, None..
S. Williams, None..
C. Espinoza, None..
C. Tindle, None..
G. Katkar, None..
S. Sinha, None.