PO.TB06.01 · 肿瘤生物学
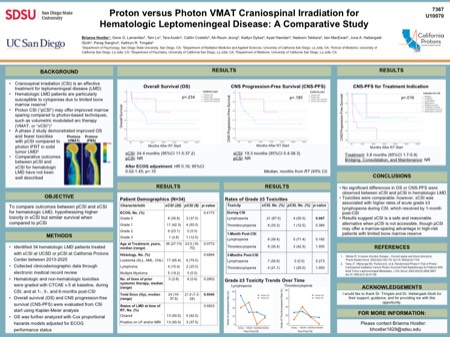
Proton versus photon VMAT craniospinal irradiation for hematologic leptomeningeal disease: A comparative study
作者与单位 Authors & Affiliations
摘要 Abstract
Craniospinal irradiation (CSI) is an effective treatment option in the treatment of hematologic leptomeningeal disease (LMD), a challenging condition seen in a variety of hematologic malignancies. Comparative outcomes between CSI delivered with protons (“pCSI”) versus modern photon-based volumetric modulated arc therapy (VMAT, or “xCSI”) have not been described in hematologic LMD. It is hypothesized that pCSI may reduce hematologic toxicity compared to xCSI due to the more favorable dose distribution regarding bone marrow sparing. This study compares acute toxicities and survival between xCSI and pCSI, hypothesizing higher toxicity with xCSI but similar survival after adjusting for performance status. Adult hematologic LMD patients treated with CSI between 2020 and 2025 were identified. Acute hematologic toxicities were graded using CTCAE v.5.0 at baseline, during treatment, and at 1- and 3-months post-CSI. Overall survival (OS) and CNS progression-free survival (CNS-PFS) were evaluated from CSI end to death and progression event, respectively, using Kaplan-Meier. OS was further analyzed using Cox proportional hazards models adjusted for ECOG performance status. Of 34 patients (median age 38), 26 (76%) received xCSI and 8 (24%) received pCSI. The delivered radiation dose ranged from 7.2 Gy-30.6 Gy in 4-17 fractions. Baseline clinicodemographic variables were similar between pCSI and xCSI: most patients had an ECOG score of 1 (p=.802), and acute lymphoblastic leukemia (58.8%) and non-Hodgkin lymphoma (17.6%) were the most common histologies (p=.517). Grade ≥3 lymphopenia was significantly higher during xCSI (p=0.006) but resolved by the 1-month post-CSI follow-up (p=.202). No other significant differences in acute hematologic toxicities were observed. Median OS was 28.3 months and did not significantly differ between the groups (28.26m; 95%CI, 21.19-35.33; p=.228) and remained nonsignificant after adjustment for ECOG (HR 0.16; 95% CI, 0.02-1.45; p=.103). Median CNS-PFS was not reached (p=.212). pCSI and xCSI demonstrated similar survival and acute hematologic toxicity profiles in hematologic LMD, supporting the safety of VMAT xCSI. However, patients who received xCSI were more likely to have severe lymphopenia, which is a particularly relevant endpoint for patients with hematologic malignancies who often have vulnerable bone marrow. These data are important to add to the existing literature on CSI for solid tumor LMD, as hematologic malignancies are a particularly at-risk population. While this study is limited by small cohort size and patient selection, it is an important first step toward optimizing the management of hematologic LMD.
利益披露 Disclosure
B. Hostler, None..
G. Lamanilao, None..
T. Le, None..
T. Austin, None..
C. L. Costello, None..
A. Jeong, None..
K. Dykes, None..
A. Hamdan, None..
N. Tabbara, None..
I. Macewan, None..
J. A. Hattangadi-Gluth, None..
P. Sanghvi, None..
K. R. Tringale, None.