PO.CL01.08 · 临床研究
Tumor-informed circulating tumor DNA dynamics reflect aggressive histology and radiologic disease status in renal cell carcinoma
作者与单位 Authors & Affiliations
摘要 Abstract
Introduction: Circulating tumor DNA (ctDNA) enables minimally invasive monitoring of tumor biology and treatment response. Although ctDNA is increasingly used across malignancies, its utility in renal cell carcinoma (RCC) has not been well established. We sought to understand the relationship between ctDNA, tumor histology, and clinical outcomes in locally advanced (laRCC) and metastatic RCC (mRCC).
Methods: Forty-eight patients with laRCC and mRCC underwent serial plasma ctDNA testing with a commercially available, tumor-informed assay (Signatera). Tissue from each patient's tumor was sequenced to identify individualized variants, which were then used to construct a personalized tumor-informed ctDNA assay. Serial plasma testing quantified these patient-specific variants to assess ctDNA dynamics alongside interval imaging. Associations between baseline ctDNA status, peak level of ctDNA in mean tumor molecules per milliliter (MTM/mL), histologic subtype, aggressive morphologic features (sarcomatoid, rhabdoid, necrosis), and radiologic findings were analyzed. Quantitative variables were compared using Kruskal-Wallis and Mann-Whitney U tests. Survival was evaluated using Kaplan-Meier and log-rank testing.
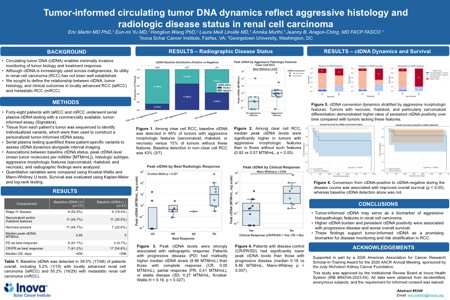
Results: ctDNA was detected at baseline in 39.5% (17/48) of patients overall, including 5.2% (1/19) with laRCC and 55.2% (16/29) with mRCC. Among clear cell (cc) RCC, baseline ctDNA was detected in 66% of cases with aggressive morphologic features (sarcomatoid, rhabdoid, or necrosis) versus 15% of clear cell tumors without these features. Baseline detection in non-clear cell RCC was 42% (3/7). Among ccRCC, the median peak ctDNA level was significantly higher in tumors with aggressive features compared to those without (0.82 vs 0.07 MTM/mL, p < 0.05). Peak ctDNA levels were strongly associated with radiologic disease status: patients with progressive disease (PD) had markedly higher median ctDNA levels (8.86 MTM/mL) compared with those demonstrating disease control with complete response (CR, 0.00 MTM/mL), partial response (PR, 0.41 MTM/mL), or stable disease (SD, 0.27 MTM/mL; H = 9.16, p = 0.027). When stratified by disease control (CR/PR/SD) versus disease progression (PD), patients with disease control exhibited significantly lower peak ctDNA levels (median 0.18 MTM/mL, n = 12) than those with progression (median 8.86 MTM/mL, n = 8; p = 0.007). Conversion from ctDNA-positive to ctDNA-negative during the disease course was associated with improved overall survival (p < 0.05). However, baseline ctDNA detection alone did not correlate significantly with survival.
Conclusions: ctDNA may serve as a predictor of aggressive histopathologic features in RCC. Quantitative burden and ctDNA dynamics appear associated with disease status and overall survival. These findings highlight tumor-informed ctDNA as a promising biomarker in RCC.
利益披露 Disclosure
E. Martin, None..
E. Yu, None..
A. Murthi, None..
H. Wang, None..
L. Linville, None..
J. B. Aragon-Ching, None.