PO.CL07.01 · 临床研究
Exploring the impact of RAS mutations in abdominopelvic Rosai Dorfman disease on responsiveness to targeted therapies: A case control study
作者与单位 Authors & Affiliations
摘要 Abstract
Introduction: Rosai Dorfman Disease (RDD) is a non-Langerhans cell histiocytic neoplasm characterized histologically by S100, CD68 and CD163 positive sinus histiocytosis with variable emperipolesis. Abdominopelvic RDD represents a rare disease subtype, for which the molecular landscape and associated responses to targeted therapies remain poorly characterized.
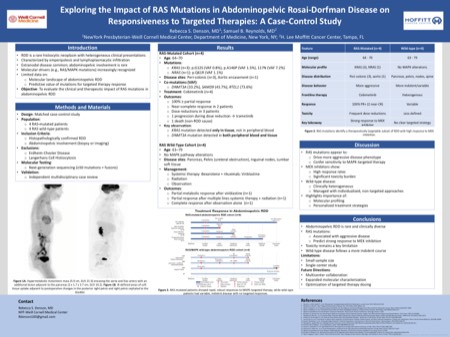
Methods: We conducted a single-center matched case-control study comparing 4 patients with RAS- mutated multifocal abdominopelvic RDD to 4 with RAS wild-type disease. All patients had confirmed histopathologic diagnoses of RDD with evidence of abdominopelvic disease, confirmed by either direct lesional biopsy or imaging demonstrating extension from a primary extra-abdominal site. Comprehensive genomic profiling was performed for each patient using a next-generation sequencing platform capable of detecting at least 50 mutations and/or fusions. Independent case review was conducted by a panel of investigators to validate diagnoses, molecular findings, and disease localization.
Results: Four similarly aged patients (64-70 years) with RAS- mutated abdominopelvic RDD (3 with KRAS mutations, 1 with NRAS mutation) were evaluated at a single center. Disease localization included peri-colonic soft tissues in 3 patients and with encasement of the abdominal aorta in one patient. Two patients were also diagnosed with clonal hematopoiesis of indeterminate potential, one each respectively harboring DNMT3A and RTEL1 mutations. All 4 patients received frontline cobimetinib with 3 achieving at least a partial response and two demonstrating near-complete resolution of all known disease sites. Dose attenuations were required in three patients due to toxicities. One patient eventually progressed during dose reduction and was transitioned to trametinib; another passed from non-RDD cardiac causes.
We also reviewed an age-matched cohort (63-79) of 4 patients with abdominopelvic RDD lacking baseline RAS/MAPK pathway or other driver mutations. Lesions were collectively identified in the pancreas, lower pelvis, inguinal lymph nodes and soft tissues proximal to the lumbar spine. Management strategies varied as only two patients received frontline systemic therapy, one sequentially with bexarotene followed by rituximab and the other with vinblastine. Three patients underwent radiation during their disease course, one as monotherapy for localized disease and two in consolidation following the systemic therapy. The remaining patient was observed off treatment.
Conclusions: Patients with RAS - mutated abdominopelvic RDD tend to experience a more aggressive disease course compared to wildtype but demonstrate marked sensitivity to MAP Kinase pathway-targeting therapies. The findings of this study are limited by small sample size; ongoing efforts are underway to expand with a multi-center cohort.
利益披露 Disclosure
R. Denson, None..
F. Amisha, None..
D. Pottinger, None..
L. Zhang, None..
L. Sokol, None..
S. B. Reynolds, None.