PO.CL01.12 · 临床研究
Spatially resolved tumor-cell MHC class II shapes adaptive immunity and therapeutic response in triple-negative breast cancer
作者与单位 Authors & Affiliations
摘要 Abstract
Background: MHC class II molecules are normally restricted to professional antigen-presenting cells. Prior TNBC studies have focused on immune-compartment MHC-II. Using spatial transcriptomics, we recently identified aberrant tumor-cell MHC-II expression. Here, we characterized the immune architecture surrounding HLA-DRA-expressing tumor cells.
Methods: High-plex single-cell spatial transcriptomics (CosMx TM SMI) was performed on treatment-naïve TNBC (Mayo TMA, n=65) and two neoadjuvant pembrolizumab cohorts (Mayo n=8; Emory n=4). Spatial neighborhoods were mapped relative to HLA-DRA-high tumor cells. Differential expression and adaptive immune gene-set scores were evaluated. Clinical relevance was assessed using FinXX (n=114), I-SPY2 (n=364), and Caris CODEai (n=3,662).
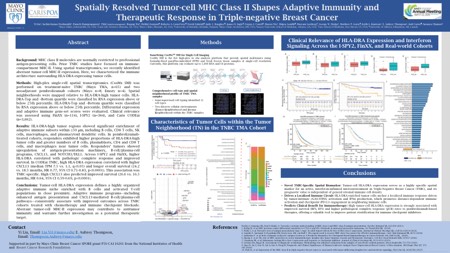
Results: HLA-DRA-high tumor regions showed significant enrichment of adaptive immune subsets within ≤50 μm, including B cells, CD8 + T cells, NK cells, macrophages, and plasmacytoid dendritic cells. In pembrolizumab-treated cohorts, responders exhibited higher proportions of HLA-DRA-high tumor cells and greater numbers of B cells, plasmablasts, CD4 + and CD8 + T cells, and macrophages near tumor cells. Responders' tumors showed upregulation of antigen-presentation machinery, B-cell/plasma-cell programs, CXCL13, and NOTCH3/DLL1. Across I-SPY2 and FinXX, higher HLA-DRA correlated with pathologic complete response and improved survival. In CODEai TNBC, high HLA-DRA expression correlated with higher CXCL13 (median TPM 7.5 vs. 1.1, q<0.05) and longer overall survival (24.2 vs. 18.5 months, HR 0.77, 95% CI 0.71-0.83, p<0.0001). This association was TNBC-specific. High CXCL13 also predicted improved survival (26.6 vs. 16.5 months, HR 0.64, 95% CI 0.59-0.69, p<0.0001).
Conclusions: Tumor-cell HLA-DRA expression defines a highly organized adaptive immune niche enriched with B cells and activated T-cell populations in close proximity. Adaptive immune programs-including enhanced antigen presentation and CXCL13-mediated B-cell/plasma-cell pathways-consistently associate with improved outcomes across TNBC cohorts treated with chemotherapy and immune checkpoint blockade. Aberrant tumor-cell MHC-II expression may contribute to antitumor immunity and warrants further investigation as a potential therapeutic target.
利益披露 Disclosure
Y. Liu, None..
S. K. Deshmukh, None..
T. Susiriwatananont, None..
B. Wu, None..
H. Joensuu, None..
S. Wu, None..
S. Gandhi, None..
M. Lustberg, None..
G. W. Sledge, None..
E. Thompson, None..
J. Carter, None.
S. Chumsri,
Merck ).
Pfizer ), Other, Consulting fee.
Genentech ), Other, Consulting fee.
Menarini Stemline Other, Consulting fee.
Seagen Other, Consulting fee.
Eisai Other, Consulting fee.
Puma Other.
AstraZeneca/Daiichi Other, Consulting fee.